At Senior Care Solutions, we often find that facilities aren’t underperforming because they lack clinical skill.
They’re underperforming because they’re not capturing what they are already doing.
PDPM is a documentation and systems model. If it’s not documented correctly, it doesn’t count.
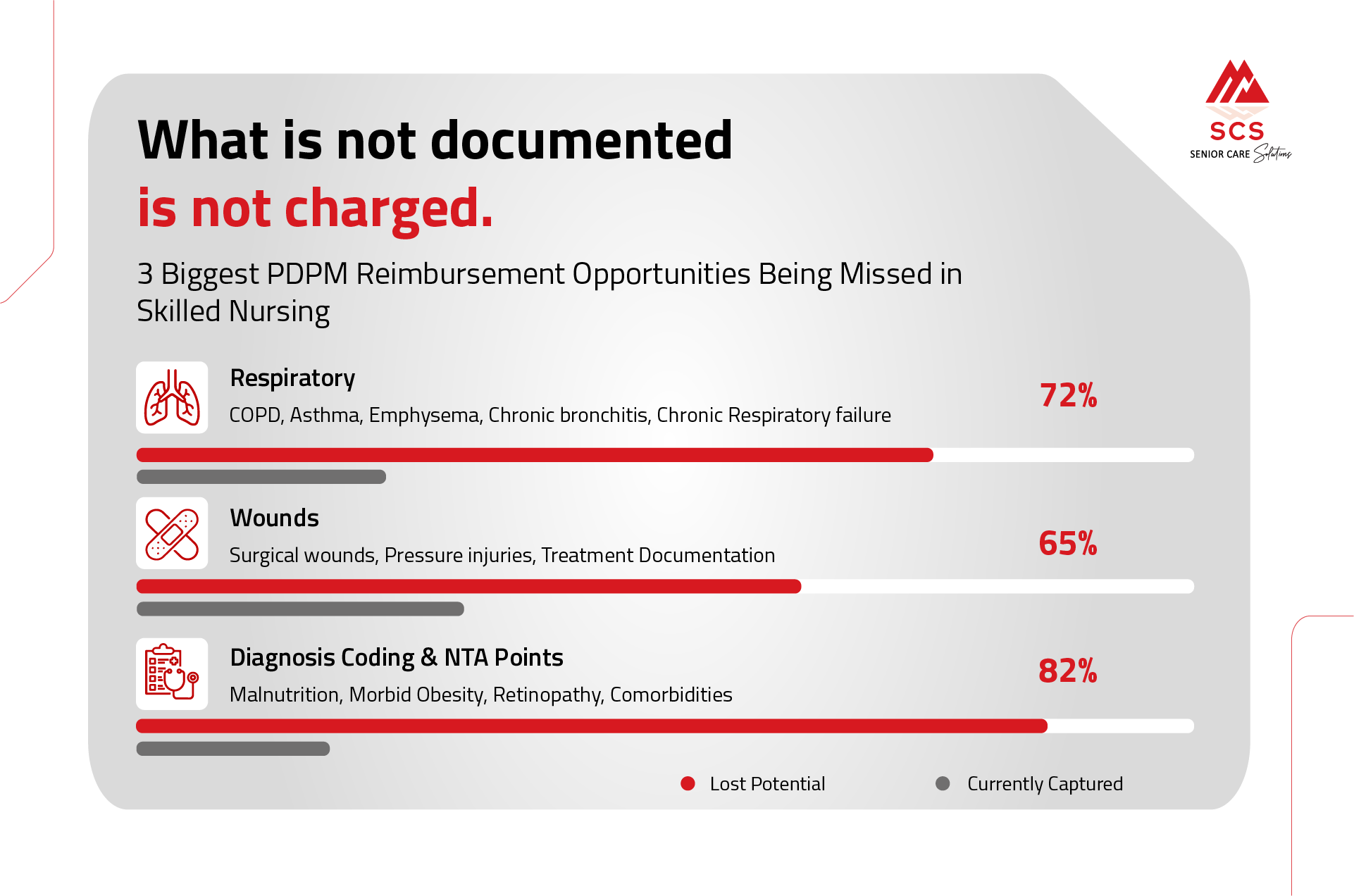
Here are the most common reimbursement opportunities we see being missed in both PDPM State Case Mix and Medicare PDPM.
Respiratory is one of the biggest missed reimbursement drivers, especially in long-term care.
What is being missed?
✔ Chronic Lung Diagnoses + Shortness of Breath with Head of Bed Elevated
Many residents cannot lie flat due to breathing discomfort… but it’s never documented during the ARD window.
If:
NOTE: That must be documented and work with provider to determine if it is tied to a respiratory diagnosis.
✔ Respiratory Therapy (Nebulizer Treatments)
If it isn’t clearly documented and minutes are not captured, it does not count.
Simple Tool to Implement:
From our Recipe for Reimbursement framework :
2. Wounds: Documentation That Leaves Money on the Table
Wound reimbursement is often missed due to incomplete documentation - not lack of treatment.
Common Misses:
If the wound is present, treated, and active -it must be documented precisely.
PDPM is diagnosis + treatment driven.
Simple Wound Capture Tool:
During weekly MDS review:
3. Diagnosis Coding & NTA Points: The Silent Revenue Driver
This is one of the most overlooked areas in both Medicare and Case Mix.
Section I: Choosing the Correct Primary Diagnosis
The primary diagnosis must:
Incorrect primary diagnosis can significantly lower the PDPM rate.
NTA Points That Are Frequently Missed:
If it’s not coded in Section I, it does not generate NTA points.
4. Section K: Swallowing & IDT Communication
Under Medicare PDPM:
Swallowing disorders impact the SLP component.
Common gaps:
There must be:
5. Section GG: The Foundation of Case Mix & Medicare
Section GG drives:
Common issues:
From our Recipe framework :
✔ Daily GG discussions during ARD window
✔ Nurse aide point-of-care documentation
✔ Weekly IDT MDS huddles
✔ Audit dependent coding (assist of 2)
✔ Clarification note before MDS closes
Goal: Accurate ADL capture. Not inflated, accurate.
The SCS 5-Point Capture Tool
Here is a simple framework facilities can implement immediately:
Step 1: Weekly ARD Huddle
Step 2: Diagnosis Audit
Step 3: Respiratory Program
Step 4: Wound Verification
Step 5: GG Integrity
Final Thought
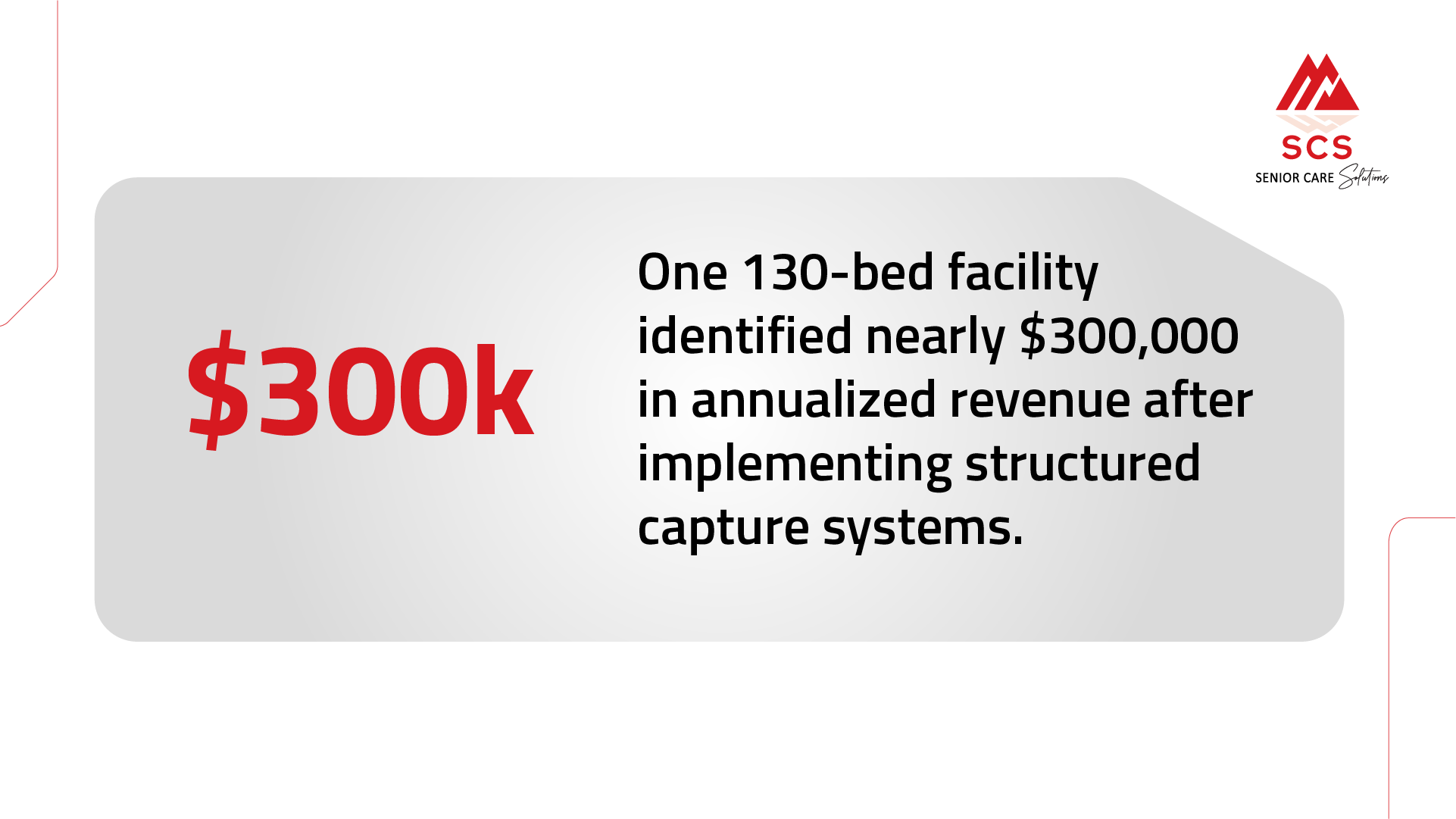
Most facilities do not have a reimbursement problem.
They have a systems capture problem.
When documentation reflects the clinical reality already happening in your building, reimbursement aligns.